![]()
Resource Library
PSI Safe Water Treatment, Products and Services
Describes PSI's work in safe water systems and household based water treatment, focusing on projects in Zambia, India, Madagascar, Tanzania and Afghanistan. An excellent summary on the need for home-based water treatment systems and products available to treat diarrhea causing agents.
Resource Type : Webinar
Country : Afghanistan, India, Madagascar, Tanzania, Zambia
Year : 2005-01-01T14:30:00
Language :
Project : SHOPS
Resource Library

Disinfecting Water, Saving Lives
A profile of point-of-use safe water products to prevent diarrhea and improve family health. Describes Safe Water Solution (SWS) and PuR, Purifier of Water and highlights PSI point-of-use water programs in 7 countries.
Resource Type : Brochure/Postcard
Country : Haiti, India, Kenya, Madagascar, Malawi, Tanzania, Zambia
Year : 2005-10-01T12:00:00
Language :
Project : SHOPS
Resource Library

PSI Public-Private Partnership in Tanzania for Net Delivery
SMARTNET is a public/private partnership between the Ministry of Health (MOH), PSI/Tanzania, net manufacturers, insecticide suppliers, distributors, wholesalers, retailers, NGOs, research organisations, advertising and promotion companies, the UK Department for International Development (DFID) and the Royal Netherlands Embassy. SMARTNET is preventing malaria in Tanzania by building a sustainable market for Insecticide Treated Nets (ITNs) whilst ensuring equitable access for the most vulnerable. SMARTNET is managed by PSI/Tanzania and funded by DFID and the Royal Netherlands Embassy.
Resource Type : Brief
Country : Tanzania
Year : 2005-05-01T12:00:00
Language : English
Project : SHOPS
Resource Library
Cost-effectiveness of zinc as adjunct therapy for acute childhood diarrhoea in developing countries
Presents a cost-effectiveness analysis in terms of DALYs and child deaths averted using a simluation technique with cost data from health facilities in Tanzania. The authors concluded that zinc was highly cost effective and there was sufficient evidence to recommend the includion of zinc into standard case amangemetn of both dysenteric and non-dysenteric acute diarrhoea.
Resource Type : Other
Country : Tanzania
Year : 2004-07-01T15:30:00
Language : English
Project : SHOPS
Resource Library
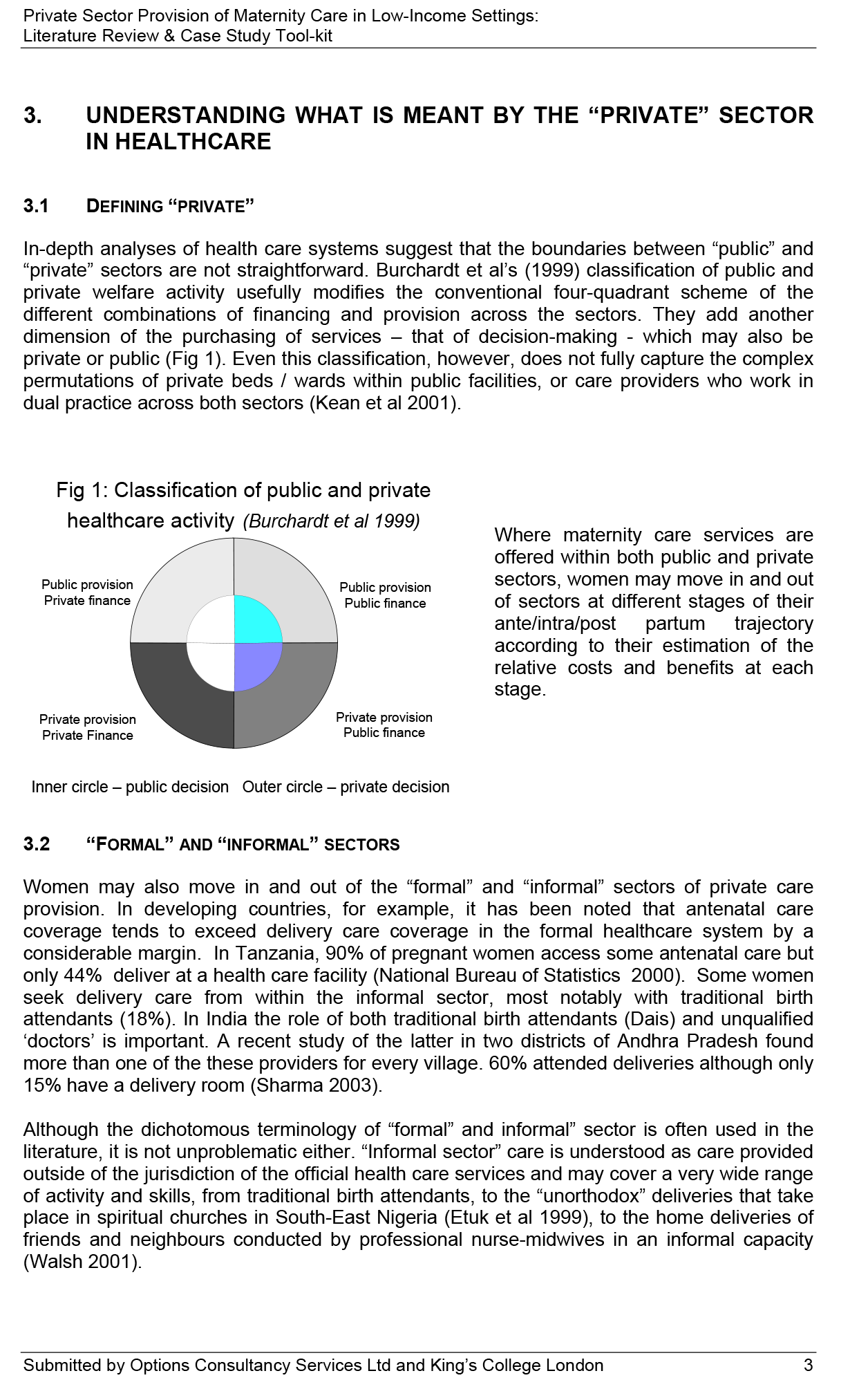
Examining the Role of Private Maternity Services in Nepal, India and Tanzania
The maternal and child millennium development goals (MDG) call for a reduction of maternal mortality by three-quarters and child deaths by two-third between 1990 and 2015. It is widely acknowledged that a functioning healthcare system is essential to achieve these aims. To date, Maternal and Newborn Health (MNH) initiatives have primarily focused on improving skills, resources, and referral systems within public sector services. The private maternity care sector has received little attention. However, in many low income countries, there is reportedly a growth in the non-government provision of maternity and obstetric care, and health sector reform strategies are promoting private and public sector "mixes". If the ambitious targets set for reduction in maternal and child health are to be reached, the role played by different elements within the private sector, their limitations and their capacity, and their interface with government services in key areas such as skilled attendance and essential obstetric care, all need to be far better understood. This literature review brings together existing knowledge concerning private (non-government) sector maternity care provision in low-income settings and identifies some key issues for future exploration. It presents a set of tools designed to gather information about private sector provision of maternity care at National or sub-National levels. These tools were simultaneously piloted in three settings, the State of Andhra Pradesh in India, Nepal and Tanzania. Separate reports from each of these pilot studies have been prepared (Ensor & Dey 2003; MacDonagh & Neupane 2003 and Murry & Nyambo 2003). A synthesis report that draws out the key issues arising from this review and across the three settings is also available (MacDonagh, Murray and Ensor 2003). Section 2 explains the scope of and methods used in the review of the literature. Section 3 provides an introduction to some of the terminology and typologies used in discussion of the "private " healthcare sector. Section 4 outlines the findings of the literature review on private sector maternity care in developing countries, and Section Five draws out five key areas where further investigation is required. In section 6 examples of existing initiatives in work with private sector providers of maternity care are outlined. Section 7 introduces a "tool kit" designed to assist local study of private sector provision of maternity care, and the annexes contain the pilot-tested tools.
Resource Type : Tool
Country : India, Nepal, Tanzania
Year : 2003-12-12T10:00:00
Language : English
Project : SHOPS
Resource Library

Obstacles to Quality of Care in Family Planning and Reproductive Health Services in Tanzania
Issues of quality of care have become central in debates about family planning and provision of reproductive health services. These debates are a response to inequalities that have not historically been captured in service delivery studies. Discussions concerning quality of care, and my arguments in this paper are an attempt to address crucial health care issues that lie behind the numbers of condoms distributed and sterilizations performed such as how well family planning programs serve the needs of clients, both technically and interpersonally. The analysis of quality of care in this paper relies on the definition provided by Hardon and Hayes (1997) in their expanded version of the commonly accepted Bruce (1990) framework. This framework hypothesizes that quality of care is composed of the following seven elements: choice of methods, information given to clients, technical competence, client-provider interpersonal relations, mechanisms to encourage continuity, appropriate constellation of services, and avoidance of incentives and disincentives.
Resource Type : Other
Country : Tanzania
Year : 1998-08-31T15:00:00
Language : English
Project : SHOPS
Resource Library
Challenging Inequities in Health: from ethics to action
This volume, Challenging Inequities in Health, was conceived as a response to the following: Concerns about widening "health gaps" both between and within countries; disproportionate research focus on inequalities in health in the "North" to the relative neglect of the "South"; and inadequate analytic tools and pragmatic policies to redress health inequities. Through a collective effort of researchers and practitioners called the Global Health Equity Initiative (GHEI), a set of in-depth country studies and conceptual analyses on health equity were undertaken. The main findings of this effort are presented in this book with the central claim that issues of equity, or distributive justice, deserve primary consideration in health and social policy deliberations. Insights about health equity from the fields of epidemiology, demography, economics and other disciplines are brought to life in case studies from Bangladesh, Chile, China, Japan, Kenya, Mexico, Russia, South Africa, Sweden, Tanzania, the United Kingdom, the United States and Vietnam. The subject matter ranges from adolescent livelihoods in Tanzania to the health burden of peoples living in marginalized counties in Mexico, from the historical antecedents of health equity in Japan to the recent increase in the gender gap in life expectancy in Russia. As a group, the studies point unambiguously to the existence and multiple dimensions of inequities in health around the globe—in rich and poor countries alike.
Resource Type : Report
Country : Kenya, Russia, South Africa, Tanzania, Vietnam
Year : 1999-11-30T00:00:00
Language : English
Project : SHOPS
Resource Library
Quality and Comparison of Antenatal Care in Public and Private Providers in the United Republic of Tanzania
In recent years, many developing countries have been actively seeking to improve the outputs and outcomes of their health care delivery system by engaging in a process of reform. The present study, carried out in Dar es Salaam in 1999, compared the quality of antenatal care offered by public and private providers at the first-tier level.
Resource Type : Other
Country : Tanzania
Year : 2003-08-23T10:15:00
Language : English
Project : SHOPS
Resource Library
Socially marketed insecticide-treated nets to improve malaria and anaemia in pregnancy in southern Tanzania
OBJECTIVES To study the uptake of socially marketed insecticide-treated nets (ITNs) and their impact on malaria and anaemia in pregnancy; and to report on a discount voucher system which aimed to increase coverage in pregnancy. METHODS A 12-month cross-sectional study of women in the second or third trimester of pregnancy. ITN use and other factors were assessed by questionnaire and a blood sample taken for malaria parasitaemia and anaemia. `Non-users' of ITNs included both women not using any net and women using untreated nets. RESULTS Fifty three per cent of pregnant women used ITNs. Women aged 15±19, primigravidae, unmarried women, and those with no access to cash had the lowest ITN use. Fewer ITN users were positive for malaria than ITN non-users (25 vs. 33%: P 0.06), and the protective efficacy (PE) for parasitaemia was 23% (CI 2±41). Multiparous ITN users had a twofold decrease in parasite density compared with multiparous non-ITN users (625parasites/ll vs. 1173 parasited/ll: P 0.01). Fewer ITN users were anaemic (Hb < 11 g/dl) than ITN non-users (72 vs. 82%: P 0.01). ITNs had a PE of 12% (CI 2±21) against mild anaemia and a PE of 38% (CI 4±60) against severe anaemia (Hb < 8 g/dl). There was a trend in the prevalence of severe, mild and no anaemia, and of high density, low density and no malaria infection by ITN status. Recently treated nets were most effective at preventing malaria and anaemia (prevalence of mild anaemia was 68% compared with 82% for those without nets (P 0.002); prevalence of malaria was 22% compared with 33% for those without nets (P 0.02). Knowledge and reported use of the discount voucher system were low. Further qualitative research is ongoing. CONCLUSIONS A modest impact of ITNs on pregnancy malaria and anaemia was shown in our high malaria transmission setting. The development of ITN programmes for malaria control should include pregnant women as a specific target group.
Resource Type : Other
Country : Tanzania
Year : 2002-02-01T14:30:00
Language : English
Project : SHOPS
Resource Library
Cost-Effectiveness of Social Marketing of Insecticide-Treated Nets for Malaria Control in the United Republic of Tanzania
Objective To assess the costs and consequences of a social marketing approach to malaria control in children by means of insecticidetreated nets in two rural districts of the United Republic of Tanzania, compared with no net use. Methods Project cost data were collected prospectively from accounting records. Community effectiveness was estimated on the basis of a nested case–control study and a cross-sectional cluster sample survey. Findings The social marketing approach to the distribution of insecticide-treated nets was estimated to cost US$ 1560 per death averted and US$ 57 per disability-adjusted life year averted. These figures fell to US$ 1018 and US$ 37, respectively, when the costs and consequences of untreated nets were taken into account. Conclusion The social marketing of insecticide-treated nets is an attractive intervention for preventing childhood deaths from malaria.
Resource Type : Brief
Country : Tanzania
Year : 2003-01-01T14:00:00
Language : English
Project : SHOPS