![]()
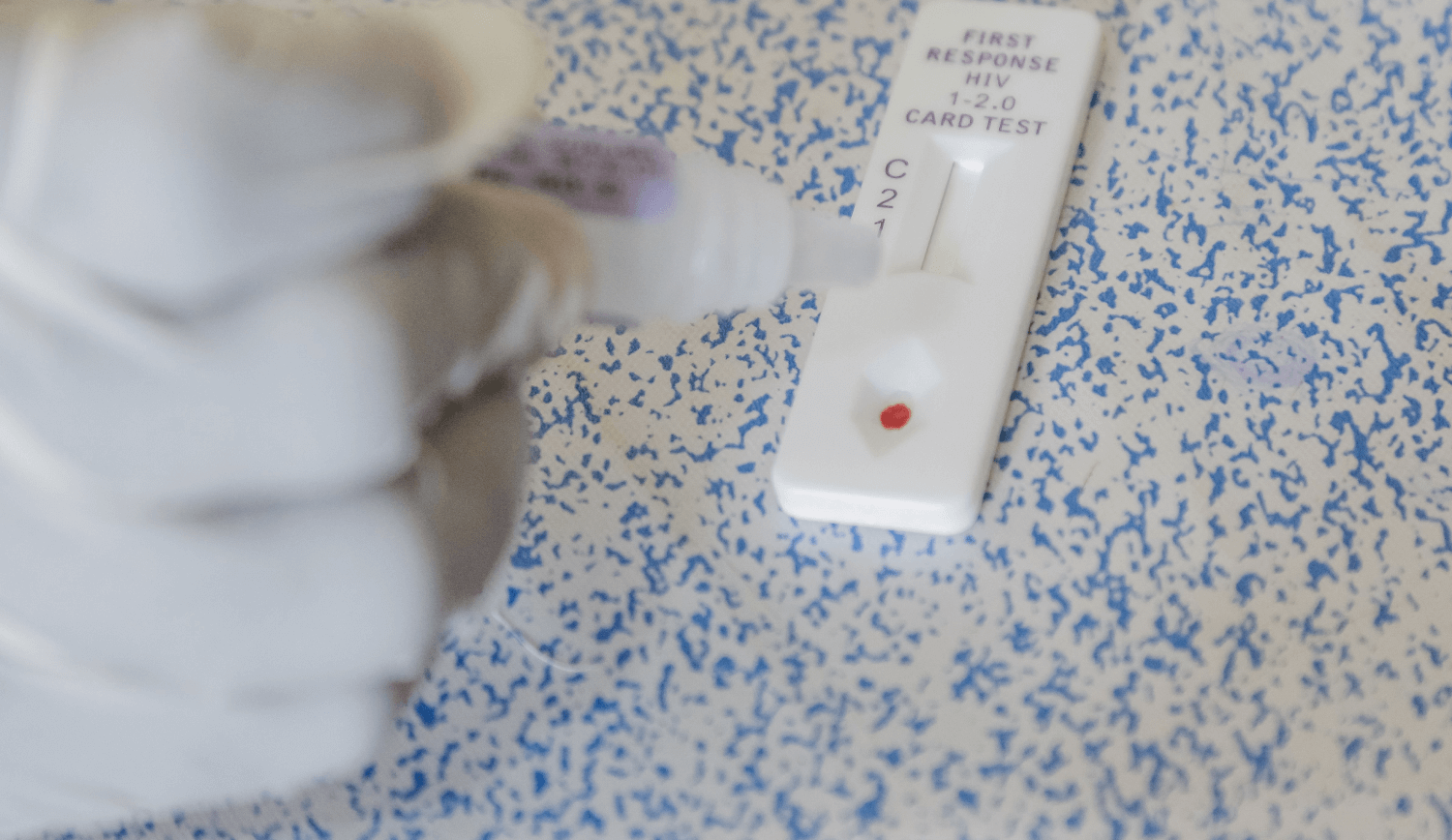
Applying the Market Development Approach to Strengthen HIV Self-Testing Markets

Could you give us some more details on how the MDA works?
The MDA maps out all elements of market interactions across relevant market actors, thus providing a good overview of the problem statement and interactions. It has the explicit objective of creating more effective and more inclusive market systems and facilitating the role of development agencies in support of this by moving from traditional top-down technical assistance to market facilitation. This approach focuses on empowering market actors to design and deliver solutions and interventions that create effective and healthy markets for different products and services within different health areas by laying down a “pathway to impact” that involves the following stages: (1) diagnose, (2) design, and (3) deliver—while adapting and learning to maximize impact throughout the process.
How is this approach applied to the HIV self-testing market in Tanzania?
For HIV self-testing in Tanzania, FHM Engage conducted market scoping, and subsequently identified a group of different market actors from the public, private, and non-governmental sectors, and brought them together to discuss various elements of the market through a series of workshops that progressed on the pathway for impact previously mentioned.
How does this approach and its implementation differ from previous approaches used?
The MDA is a consultative process and requires collaboration with all the different market actors to co-create a vision for the market of a health product or service. It is strongly data driven. For HIV self-testing in Tanzania, the Market Development Group formed by FHM Engage developed a vision for the market where both oral and blood-based HIV self-testing kits are available with potential for other products, such as urine-based HIV self-test kits, to also be distributed when available. The HIV Self-Testing Implementation Framework developed by the Tanzania National AIDS Control Program determined the target groups and geographic areas for this implementation. The vision is to create an HIV self-testing market that is healthy and allows both public and private supply and delivery, along with supporting a total market approach that has public, socially marketed, and commercial products.
Keeping the total market in mind—free commodities from the public sector, subsidized commodities from the social marketing sector, and commercial products from the commercial sector—and leveraging insights from data enable one to think about the specific target groups and geographic areas to achieve maximum impact for those who need the health products and services the most. The challenge, however, is that since it is a systems approach the measurement is in the long term and may take some time. There are a lot of necessary pre-steps such as development of the right policies and guidelines needed before actual implementation. This is the path that FHM Engage has been taking in Tanzania.
Consumer choice often plays a key role in determining how health care resources are accessed. How does this factor influence the application of the MDA to the condoms and HIV self-testing markets in Tanzania?
The MDA works ideally through market development groups such as the one that was formed by FHM Engage in Tanzania. These groups must have market actors from both the public and the private sectors who can develop a vision for the market together. Insights and data from consumers about their preferences must be used in developing this vision and implementing the right interventions for a healthy market. We used various data sources, including work done by previous programs in the space, to understand consumer preferences and conduct our own rapid assessments with consumer target groups. We also included groups such as civil society organizations in our discussions to ensure that we can factor in the preferences of the consumers.
This story was cross-posted from Chemonics International.
Recent Highlights
-
Written by :
-
Published on : 16-Nov-23
- Highlight Type : Blog
- Country : ,
- Project : FHM Engage
- Language : English
It’s the Behaviours that Count
This post was originally published by BEAM Exchange, and is cross posted with permission.
As the project director for a new USAID-funded global flagship programme called Frontier Health Markets (FHM) Engage, you may think that I spend all my time focused on markets for family planning, maternal and child health, HIV, malaria, or TB. But you’d only be half right.
Nine months into this roller coaster ride, I find myself spending a surprising amount of time talking about behaviours.
Not the behaviours at the heart of health markets, governing the transactions between the client/patient and the provider/health worker. Nor the behaviours that are needed to support the governance of a health market in mixed health systems, as described by WHO’s recent strategy report.
Instead, I find myself talking about the operationalisation behaviours that are needed to support a global technical assistance platform like FHM Engage.
As we work across multiple markets and geographies, and from multiple angles, our consortium partners identified early on the need for common guiding principles, or behaviours, to act as the “glue” for all of our activities.
During three remotely facilitated sessions we were able to draw on more than 400 years of work experience to distil six behaviours that we deem necessary for the success of our market work:
1. Being intentional about inclusivity and equity
We defined this principle as ensuring that diverse voices of all actors are valued, incorporated, and drive implementation. In our market diagnostic work, this means including different voices – especially from the private health sector – to identify and understand the root causes for market under performance.
2. Listening before acting
We defined this as needing to first actively listen to market actors to identify root causes to problems before then co-working to identify contextually appropriate solutions. In a recent collaboration, Christopher Whitfield (Executive Director and Lead, Africa Region at Gilead) explained his team mantra as “Listen, listen, listen, listen some more, wait and reflect, and THEN act.” We couldn’t agree more.
3. Building on existing structures
We defined this as having programmes and structures, led by actors from within the market system, that are leveraged to drive scale and sustainability. To us, this behaviour is about understanding both public and private platforms, technical working groups and associations and identifying ways to add value to those structures. It means not creating duplicative structures even if such a structure might give quick wins in the near term.
4. Embracing adaptive learning
Our consortium partners defined this behaviour as having a fail-fast mindset to drive us towards creative problem solving and excellence. While failing-fast might sound high risk, within FHM Engage we think of it as making the potential solutions that we co-design visible, even tangible – something that market actors can get their arms around. We then point out challenges so that it “fails fast” and we can co-design stronger and more sustainable solutions.
5. Being persistent yet patient
We defined this as understanding that change takes time and is often met with resistance, so we need to be both brave and bold. For us, this behaviour means taking time to fully understand and operationalise what the market approach means and how it links to our traditional private sector approaches and intended areas of health impact. Understanding the distinction between a market approach and a systems approach is nuanced and yet critical for us. As we get into the work, we are committed to being persistent in asking questions, learning from others, and being patient with ourselves and market actors.
6. (Last but not least) Nurturing trust and respect
Our consortium defined this behaviour as leading with empathy, collaborating with dignity, and trusting that all market actors are capable of excellence. In our country-level work, nurturing trust and respect between public and private sector partners is critical to our success. To do this effectively, the local market actors with whom we partner will need to be neutral parties. FHM Engage will support these market actors to run strong market facilitation processes that earn respect and build trust.
In sharing these six crowd-sourced behaviours, I hope to hear from our programmes and other interventions about which behaviours they have found critical to the success of their market facilitation work.
We will be sure to report back on how the adoption of these behaviours has helped (or hindered) our work. Until then!
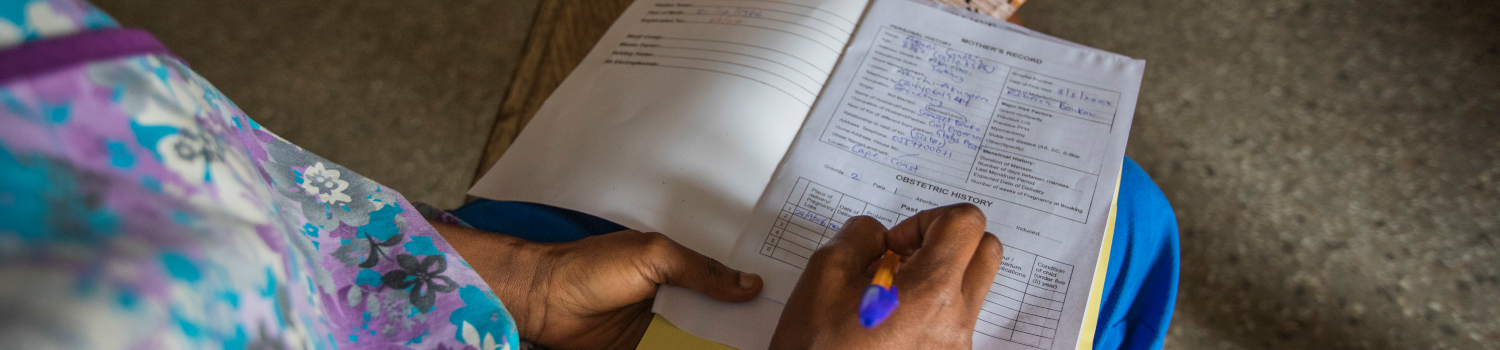
Banner image caption: Rebecca Donkor, midwife at community-based Health Planning and Services facility in Abirew, Ghana, conducts routine check-in with pregnant client Cynthia Agyei. Credit: GHSC-PSM Maternal Newborn & Child Health Task Order.
Recent Highlights
-
Written by : Cynthia Eldridge
-
Published on : 17-Aug-22
- Highlight Type : Blog
- Country :
- Project : FHM Engage
- Language : English
Resource Library
FHM ENGAGE DATA AVAILABILITY ASSESSMENT Mapping of data availability to measure the overall size of the private sector across FP2020 focus countries and comparison of existing estimates for FP market size 1.4.B
The private health sector includes all non-state actors involved in health, both for-profit and non-for-profit entities, formal and informal providers, as well as domestic and international actors. The heterogeneous private sector has been an important source of healthcare services and product provision in many low- and middle-income countries (LMICs), including family planning (FP). To facilitate an enabling environment for sustainable health transactions, particularly on FP, and maternal, newborn, and child health (MNCH), among other health products and services, it is crucial to understand the collective capacity of the private sector in providing health care services and products.
Resource Type : Report
Country : Global
Year : 2022-11-14T12:24:09
Language : English
Project : FHM Engage
Resource Library

FHM Engage Private Sector Global Data Summary
The private health sector includes all non-state actors involved in health, both for-profit and non-for-profit entities, formal and informal providers, as well as domestic and international actors. The heterogeneous private sector has been an important source of healthcare services and product provision in many low- and middle-income countries (LMICs), including family planning (FP). To facilitate an enabling environment for sustainable health transactions, particularly on FP, and maternal, newborn, and child health (MNCH), among other health products and services, it is crucial to understand the collective capacity of the private sector in providing health care services and products.
Resource Type : Report
Country : Global
Year : 2022-11-03T12:02:28
Language : English
Project : FHM Engage
Resource Library

Des marchés sains pour une population en bonne santé
FHM Engage est convaincu que le développement des marchés dans le secteur de la santé permettra d'améliorer les résultats en santé. Nous adoptons une approche systémique pour identifier les causes profondes des marchés les moins performants. Nous concevons en partenariat avec des acteurs locaux, des solutions durables afin d'apporter un changement de comportement durable nécessaire à l'évolution des marchés de la santé.
Resource Type : Brief
Country : Global
Year : 2022-10-04T09:23:14
Language : French
Project : FHM Engage
Resource Library
Healthy Markets for Healthy People
FHM Engage believes that strengthening health markets will lead to improved health outcomes. We use a systems approach to identify root causes of underperforming markets. We co-design sustainable solutions with local market actors to deliver the lasting behavior change needed to evolve health markets.
Resource Type : Brief
Country : Global
Year : 2022-05-10T13:25:15
Language : English
Project : FHM Engage
Resource Library
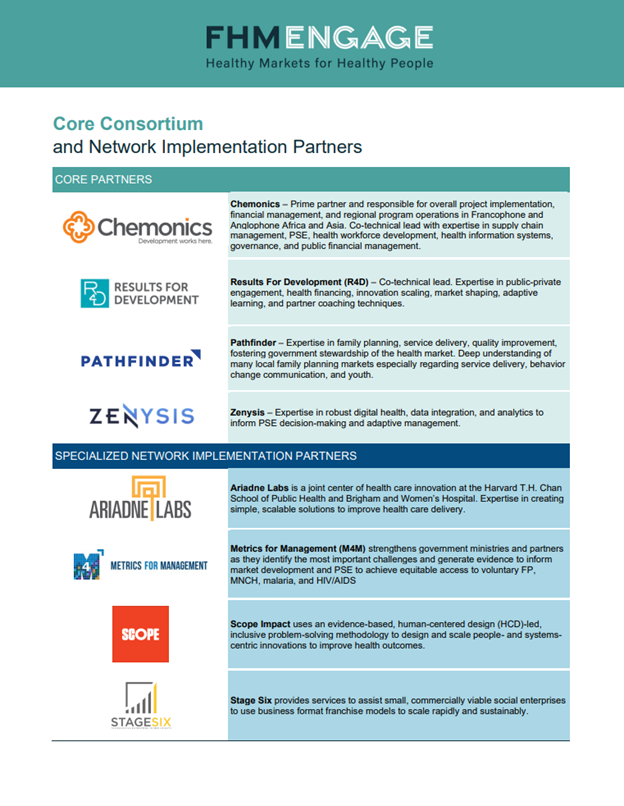
Core Consortium and Network Implementation Partners
Prime partner and responsible for overall project implementation, financial management, and regional program operations
Resource Type : Brief
Country : Global
Year : 2023-02-01T13:23:46
Language : English
Project : FHM Engage
Resource Library
Estimates of Progress
In recent years, the Track20 Project has made great strides in increasing the use of routine data to inform progress in modern contraceptive prevalence. This data is used to inform annual estimates of progress published in Family Planning 2020’s annual progress report. In the 2018 progress report, 13 countries used service statistics to help inform their current progress. Generally, countries include service delivery or commodity statistics provided through the public sector and some through NGO partners using the Estimated Modern Use tool. To account for the remaining private sector statistics, countries generally use a methodology developed by Track20 using Demographic and Health Survey data. This document explores potential alternatives to this approach by including private sector sales data into the Estimated Modern Use tool.
Resource Type : Brief
Country : Global
Year : 2019-12-10T15:39:00
Language : English
Project : SHOPS Plus
Resource Library
Sources for Sick Child Care in 24 USAID Priority Countries
Both the public and private sectors are important sources of care for sick children, and their role varies across contexts and socioeconomic statuses. Understanding if and where sick children are taken for care is critical to improve case management interventions. This brief presents a secondary analysis of Demographic and Health Survey data from 24 of the 25 USAID maternal and child survival priority countries to examine where treatment or advice is sought for sick children who experienced at least one of three treatable illnesses: fever, acute respiratory infection, or diarrhea. These illnesses represent some of the leading causes of death in children under five years old.
Resource Type : Brief
Country : Global
Year : 2018-07-09T00:00:00
Language : English
Project : SHOPS Plus
Resource Library
Is Household Wealth Associated With Use of Long-Acting Reversible and Permanent Methods of Contraception? A Multi-Country Analysis
As programs continue to expand access to family planning information, services, and products, it is critical that these efforts be undertaken with an equity lens, ensuring that regardless of socioeconomic status, all women and couples can use the method that meets their needs. This study explores the relationship between household wealth and the use of long-acting and permanent methods (LAPMs) versus short-acting methods of contraception among modern method users, using multivariate analyses based on Demographic Health Survey data from 30 developing countries conducted between 2006 and 2013. Overall, and controlling for relevant individual and household characteristics including age, number of living children, education, and urban/rural residence, we found that wealthier women were more likely than poorer women to use LAPMs instead of short-acting methods: 20 of the 30 countries showed a positive and statistically significant association between wealth and LAPM use. For 10 of those countries, however, LAPM use was significantly higher only for the top (1 or 2) wealthiest quintiles. Eight countries showed no broad pattern of association, while in 2 countries—Bangladesh and India—poorer women were more likely to use LAPMs than wealthier women. The positive association between wealth and LAPM use was found most consistently in the Latin American and the Caribbean countries in our sample. These findings can help program implementers respond better to women’s needs for modern contraception, especially in reaching women from lower- and middle-income households.
This article was published in Global Health: Science and Practice, Volume 4, No.1, pages 43-54.
Resource Type :
Country :
Year : 2016-02-17T00:00:00
Language : English
Project : SHOPS